Transcript
ReachMD Announcer:
This program is brought to you by Regeneron. The speaker is a paid consultant.
Dr. Turck:
This is Eye on Ocular Health on ReachMD, and I’m Dr. Charles Turck.
Joining me to discuss the pathophysiology and a treatment option for Macular Edema following Retinal Vein Occlusion, or RVO, is Dr. John Kitchens, on behalf of Regeneron Pharmaceuticals. Welcome to the program!
Dr. Kitchens:
Hello, Dr. Turck, and hello everyone listening. I'm Dr. John Kitchens. I'm a Retina Specialist at Retina Associates of Kentucky in Lexington, Kentucky. I'm looking forward to our conversation today.
Dr. Turck:
Well, it’s great to have you here with us, Dr. Kitchens. Before we begin, let’s take a moment to review the Indications and some Important Safety Information for EYLEA® (aflibercept) Injection 2 milligrams.
Narrator:
IMPORTANT SAFETY INFORMATION AND INDICATIONS
INDICATIONS
EYLEA® (aflibercept) Injection 2 mg is indicated for the treatment of patients with Neovascular (Wet) Age-Related Macular Degeneration (AMD), Macular Edema following Retinal Vein Occlusion (RVO), Diabetic Macular Edema (DME), and Diabetic Retinopathy (DR).
CONTRAINDICATIONS
EYLEA is contraindicated in patients with ocular or periocular infections, active intraocular inflammation, or known hypersensitivity to aflibercept or to any of the excipients in EYLEA.
WARNINGS AND PRECAUTIONS
Intravitreal injections, including those with EYLEA, have been associated with endophthalmitis and retinal detachments and, more rarely, retinal vasculitis with or without occlusion. Proper aseptic injection technique must always be used when administering EYLEA. Patients and/or caregivers should be instructed to report any signs and/or symptoms suggestive of endophthalmitis, retinal detachment, or retinal vasculitis without delay and should be managed appropriately.
Acute increases in intraocular pressure have been seen within 60 minutes of intravitreal injection, including with EYLEA. Sustained increases in intraocular pressure have also been reported after repeated intravitreal dosing with VEGF inhibitors. Intraocular pressure and the perfusion of the optic nerve head should be monitored and managed appropriately.
Dr. Turck:
To kick off our discussion, Dr. Kitchens, can you provide some background on Macular Edema following RVO and the different classifications of the disease?
Dr. Kitchens:
Yeah, absolutely.
So there are several classifications of RVO based on the site of vascular obstruction. First, Central Retinal Vein Occlusion, also known as CRVO, affects the entire retinal venous system. The occlusions localized at the lamina cribrosa of the optic disc. Branch Retinal Vein Occlusion, or BRVO, typically occurs at arteriovenous crossings. And then, Hemicentral Retinal Vein Occlusions, or HRVO, impacts one hemisphere of the fundus. The presumed site of occlusion in a Hemicentral Retinal Vein Occlusion is one of the two trunks of an abnormally split intraneural central retinal vein, and that occurs in about 20% of patients.1
Dr. Turck:
Can you also explain the pathophysiology of RVO?
Dr. Kitchens:
Sure.
[Slide on screen]
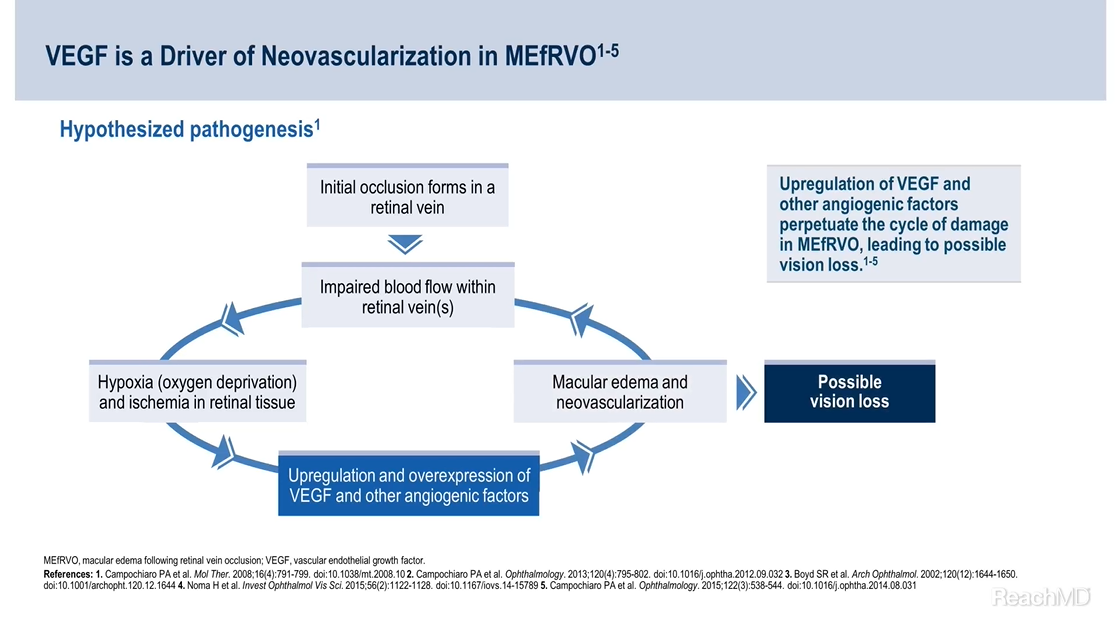
So, the development of Macular Edema following RVO is thought to begin with an occlusion in a retinal vein. What happens is this blockage impairs blood flow in the affected vascular region. This can result in hypoxia in the retinal tissues.
The lack of oxygen triggers an upregulation of VEGF, or vascular endothelial growth factor, and other pro-angiogenic factors. Consequently, this series of events can contribute to the onset of macular edema and neovascularization.2-5
Dr. Turck:
To follow up on that, what are the key drivers of RVO?
Dr. Kitchens:
[Slide on screen]
Well as mentioned earlier, overexpression of VEGF and other pro-angiogenic factors contributes to the disease progression promoting retinal nonperfusion and ischemia. And so increased levels of these factors can perpetuate Macular Edema following RVO, leading to possible vision loss.2-5
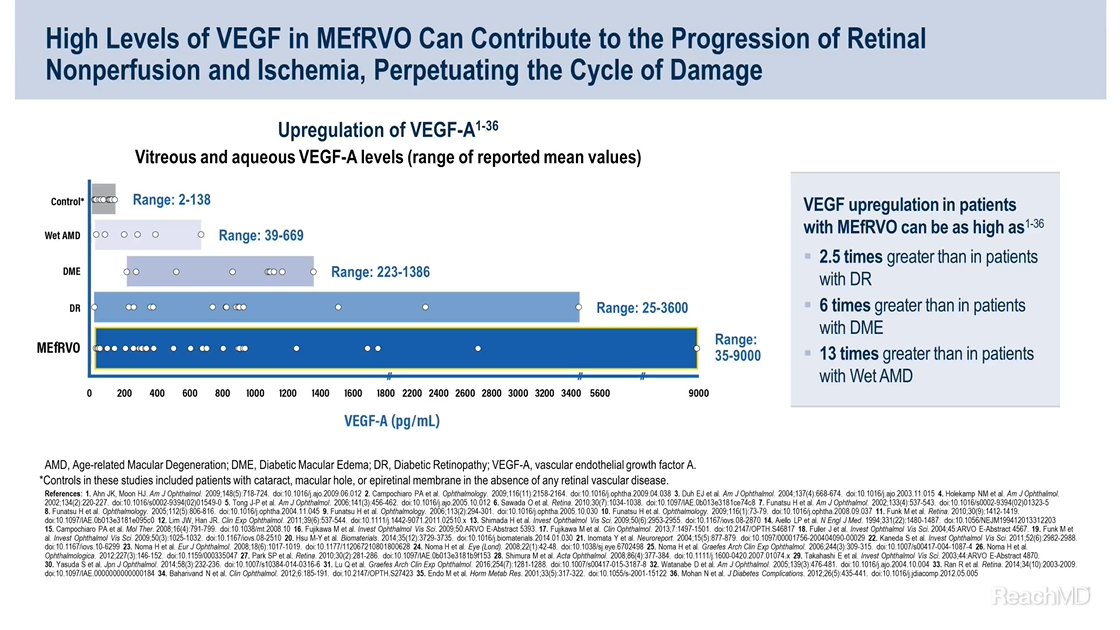
Now the elevated expression of vascular endothelial growth factor A, otherwise known as VEGF-A, in various retinal diseases has been well-documented. VEGF-A is upregulated in things like Wet AMD, Diabetic Macular Edema, and Diabetic Retinopathy, and it can be upregulated to a much greater extent in patients with Macular Edema following RVO.
In fact, several studies have shown that the expression of VEGF in patients with Macular Edema following RVO is up to 6 times greater than in patients with Diabetic Macular Edema and up to 13 times greater than in patients with Wet AMD.2,6-41
Now, it’s important to note that this graph shows ranges of mean VEGF-A levels observed in studies of VEGF-related conditions. All patients are different, of course, and this graph may not be representative of any particular patient.
Now I’d also like to note that ischemia alone may not fully account for the extent of the disease, suggesting the potential involvement of other factors in the development of Macular Edema following RVO.42
Dr. Turck:
Thank you, Dr. Kitchens for providing us with insights into the pathogenesis, classifications, and key drivers of RVO. You mentioned the potential involvement of certain other factors in the onset of Macular Edema following RVO. Could you elaborate on this?
Dr. Kitchens:
Sure. There's significant discussions within the community regarding the possible roles of other factors in the development of Macular Edema following RVO and their potential clinical relevance.42,43
[Slide on screen]
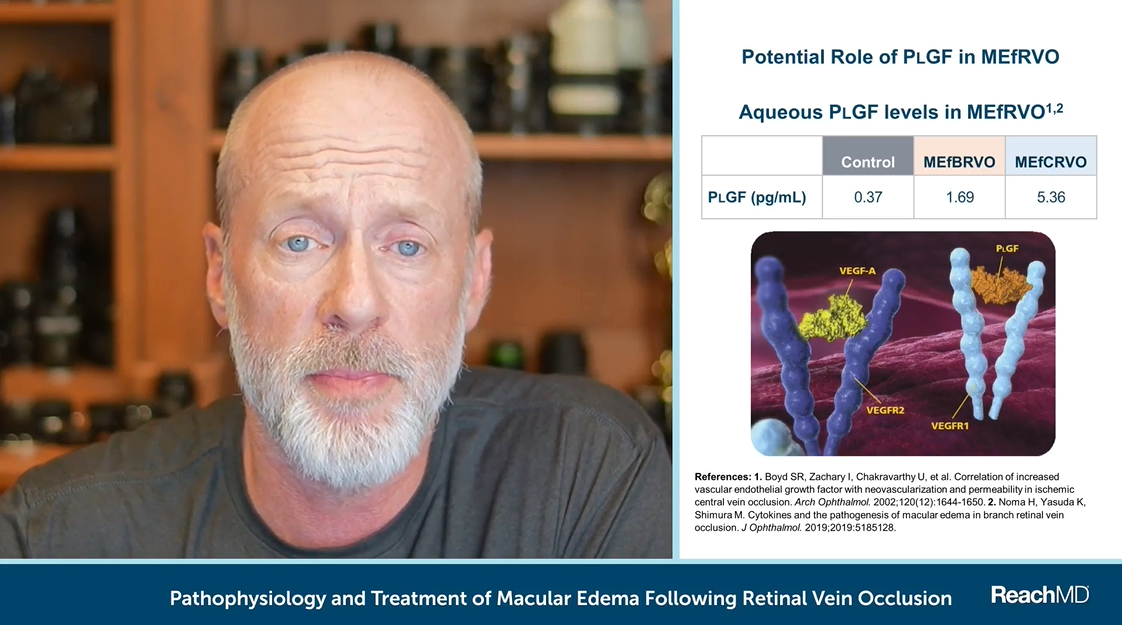
PlGF is a member of the VEGF factor family, and potentially plays a role in Macular Edema following RVO.4
Several studies have indicated elevated levels of PlGF in the aqueous humor of patients with Macular Edema following both Branch RVO and Central RVO. Compared with controls, PlGF was upregulated 4.5- and 14.5-fold in Macular Edema following Branch RVO and Central RVO, respectively.4,5,44
EYLEA® (aflibercept) Injection is the only anti-VEGF treatment for Macular Edema following RVO that also binds to PlGF.45 However, the exact role of PlGF in Macular Edema following RVO and its clinical impact is still not fully characterized and remains under investigation.5,46
Angiopoietin-2, or Ang-2, is another factor that’s been documented to be elevated in Macular Edema following RVO. Once again, the clinical impact of Ang-2 inhibition has yet to be established, and this has been acknowledged by the FDA.43,47
Dr. Turck:
So now that we better understand the background of the disease, I’d like to review some treatment options for patients with Macular Edema following RVO. But first, let’s review some more Important Safety Information for EYLEA.
Narrator:
WARNINGS AND PRECAUTIONS (continued)
There is a potential risk of arterial thromboembolic events (ATEs) following intravitreal use of VEGF inhibitors, including EYLEA. ATEs are defined as nonfatal stroke, nonfatal myocardial infarction, or vascular death (including deaths of unknown cause). The incidence of reported thromboembolic events in wet AMD studies during the first year was 1.8% (32 out of 1824) in the combined group of patients treated with EYLEA compared with 1.5% (9 out of 595) in patients treated with ranibizumab; through 96 weeks, the incidence was 3.3% (60 out of 1824) in the EYLEA group compared with 3.2% (19 out of 595) in the ranibizumab group. The incidence in the DME studies from baseline to week 52 was 3.3% (19 out of 578) in the combined group of patients treated with EYLEA compared with 2.8% (8 out of 287) in the control group; from baseline to week 100, the incidence was 6.4% (37 out of 578) in the combined group of patients treated with EYLEA compared with 4.2% (12 out of 287) in the control group. There were no reported thromboembolic events in the patients treated with EYLEA in the first six months of the RVO studies.
Dr. Turck:
With that Important Safety Information in mind, Dr. Kitchens, can you tell us about the available treatments for Macular Edema following RVO and what your treatment goals look like for these patients?
Dr. Kitchens:
Yes, so regarding treatment goals and options for Macular Edema following RVO, it's important to note that there's no single treatment to reverse occlusion and improve perfusion directly.1 As Retina Specialists, our focus is really on preserving vision, which is the most important outcome for these patients. We also aim to manage the consequences of RVO and reduce any associated edema.1,48 In addition to preserving vision, we aim for anatomical improvements such as reductions in central retinal thickness, or CRT. The safety profile of any given treatment option is also important, especially because these patients may have underlying medical conditions or comorbidities.1
Previously, laser treatment was the main intervention for Macular Edema following RVO. However, as the treatment landscape has evolved, with options such as steroids and anti-VEGF injections being more commonly used as initial therapies.1,49
As mentioned earlier, VEGF is recognized as a primary driver of the disease; therefore, anti-VEGF agents have been used for over a decade to treat Macular Edema following RVO.2-5,50
EYLEA® (aflibercept) Injection is the number one prescribed anti-VEGF that is FDA approved for Macular Edema following RVO.51 The approval of EYLEA for this indication was based on 3 robust clinical trials demonstrating the efficacy and safety of EYLEA in the treatment of Macular Edema following RVO—VIBRANT, COPERNICUS, and GALILEO studies.51,52 In our next video, we'll review the outcomes from these clinical trials.
Dr. Turck:
Thank you, Dr. Kitchens, for that informative discussion.
Let’s take a moment to review some more Important Safety Information.
Narrator:
ADVERSE REACTIONS
Serious adverse reactions related to the injection procedure have occurred in <0.1% of intravitreal injections with EYLEA including endophthalmitis and retinal detachment.
The most common adverse reactions (≥5%) reported in patients receiving EYLEA were conjunctival hemorrhage, eye pain, cataract, vitreous detachment, vitreous floaters, and intraocular pressure increased.
Patients may experience temporary visual disturbances after an intravitreal injection with EYLEA and the associated eye examinations. Advise patients not to drive or use machinery until visual function has recovered sufficiently.
Dr. Turck:
As we conclude today's session, I want to extend our sincere appreciation to Dr. Kitchens, on behalf of Regeneron Pharmaceuticals, for his invaluable insights into the pathogenesis of RVO, treatment options, and approach in using EYLEA 2 milligrams in patients with Macular Edema following RVO.
Dr. Kitchens:
Thank you, Dr. Turck.
ReachMD Announcer:
This program is brought to you by Regeneron. The speaker is a paid consultant.
References:
- Romano F, Lamanna F, Gabrielle PH, et al. Update on retinal vein occlusion. Asia Pac J Ophthalmol (Phila). 2023 Mar-Apr 01;12(2):196-210.
- Campochiaro PA, Hafiz G, Shah SM, et al. Ranibizumab for macular edema due to retinal vein occlusions: implication of VEGF as a critical stimulator. Mol Ther. 2008:16(4):791-799.
- Campochiaro PA, Bhisitkul RB, Shapiro H, Rubio RG. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology. 2013;120(4):795-802.
- Boyd SR, Zachary I, Chakravarthy U, et al. Correlation of increased vascular endothelial growth factor with neovascularization and permeability in ischemic central vein occlusion. Arch Ophthalmol. 2002;120(12):1644-1650.
- Noma H, Mimura T, Yasuda K, Shimura M. Role of soluble vascular endothelial growth factor receptor signaling and other factors or cytokines in central retinal vein occlusion with macular edema. Invest Ophthalmol Vis Sci. 2015;56(2):1122-1128.
- Ahn JK, Moon HJ. Changes in aqueous vascular endothelial growth factor and pigment epithelium-derived factor after ranibizumab alone or combined with verteporfin for exudative age-related macular degeneration. Am J Ophthalmol. 2009;148(5):718-724.e1.
- Campochiaro PA, Choy DF, Do DV, et al. Monitoring ocular drug therapy by analysis of aqueous samples. Ophthalmology. 2009;116(11):2158-2164.
- Duh EJ, Yang HS, Haller JA, et al. Vitreous levels of pigment epithelium-derived factor and vascular endothelial growth factor: implications of ocular angiogenesis. Am J Ophthalmol. 2004;137(4):668-674.
- Holekamp NM, Bouck N, Volpert O. Pigment epithelium-derived factor is deficient in the vitreous of patients with choroidal neovascularization due to age-related macular degeneration. Am J Ophthalmol. 2002;134(2):220-227.
- Tong J-P, Chan W-M, Liu DTL, et al. Aqueous humor levels of vascular endothelial growth factor and pigment epithelium-derived factor in polypoidal choroidal vasculopathy and choroidal neovascularization. Am J Ophthalmol. 2006;141(3):456-462.
- Sawada O, Miyake T, Kakinoki M , Sawada T, Kawamura H, Ohji M. Aqueous vascular endothelial growth factor after intravitreal injection of pegaptanib or ranibizumab in patients with age-related macular degeneration. Retina. 2010;30(7):1034-1038.
- Funatsu H, Yamashita H, Ikeda T, Nakanishi Y, Kitano S, Hori S. Angiotensin II and vascular endothelial growth factor in the vitreous fluid of patients with diabetic macular edema and other retinal disorders. Am J Ophthalmol. 2002;133(4):537-543.
- Funatsu H, Yamashita H, Sakata K, et al. Vitreous levels of vascular endothelial growth factor and intercellular adhesion molecule 1 are related to diabetic macular edema. Ophthalmology. 2005;112(5):806-816.
- Funatsu H, Yamashita H, Nakamura S, et al. Vitreous levels of pigment epithelium–derived factor and vascular endothelial growth factor are related to diabetic macular edema. Ophthalmology. 2006;113(2):294-301.
- Funatsu H, Noma H, Mimura T, Eguchi S, Hori S. Association of vitreous inflammatory factors with diabetic macular edema. Ophthalmology. 2009;116(1):73-79.
- Funk M, Schmidinger G, Maar N, et al. Angiogenic and inflammatory markers in the intraocular fluid of eyes with diabetic macular edema and influence of therapy with bevacizumab. Retina. 2010;30(9):1412-1419.
- Lim JW, Han JR. Aqueous humour levels of vascular endothelial growth factor and erythropoietin in patients with diabetic macular oedema before and after intravitreal erythropoietin injection. Clin Exp Ophthalmol. 2011;39(6):537-544.
- Shimada H, Akaza E, Yuzawa M, Kawashima M. Concentration gradient of vascular endothelial growth factor in the vitreous of eyes with diabetic macular edema. Invest Ophthalmol Vis Sci. 2009;50(6):2953-2955.
- Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331(22):1480-1487.
- Fujikawa M, Kakinoki M, Sawada O, Sawada T, Kawamura H, Ohji M. Vascular endothelial growth factor and retinal thickness in branch retinal vein occlusion. Invest Ophthalmol Vis Sci. 2009;50: ARVO E-Abstract 5393.
- Fujikawa M, Sawada O, Miyake T, et al. Correlation between vascular endothelial growth factor and nonperfused areas in macular edema secondary to branch retinal vein occlusion. Clin Ophthalmol. 2013;7:1497-1501.
- Fuller J, Sams W, Mason J, et al. Quantification of aqueous and vitreous VEGF following branch, hemi–, and central retinal vein occlusions. Invest Ophthalmol Vis Sci. 2004;45(13): ARVO E-Abstract 4567.
- Funk M, Kriechbaum K, Prager F, et al. Intraocular concentrations of growth factors and cytokines in retinal vein occlusion and the effect of therapy with bevacizumab. Invest Ophthalmol Vis Sci. 2009;50(3):1025-1032.
- Hsu M-Y, Yang C-Y, Hsu W-H, et al. Monitoring the VEGF level in aqueous humor of patients with ophthalmologically relevant diseases via ultrahigh sensitive paper-based ELISA. Biomaterials. 2014;35(12):3729-3735.
- Inomata Y, Hirata A, Takahashi E, Kawaji T, Fukushima M, Tanihara H. Elevated erythropoietin in vitreous with ischemic retinal diseases. Neuroreport. 2004;15(5):877-879.
- Kaneda S, Miyazaki D, Sasaki S, et al. Multivariate analyses of inflammatory cytokines in eyes with branch retinal vein occlusion: relationships to bevacizumab treatment. Invest Ophthalmol Vis Sci. 2011;52(6):2982-2988.
- Noma H, Funatsu H, Mimura T, Hori S. Changes of vascular endothelial growth factor after vitrectomy for macular edema secondary to retinal vein occlusion. Eur J Ophthalmol. 2008;18(6):1017-1019.
- Noma H, Minamoto A, Funatsu H, et al. Intravitreal levels of vascular endothelial growth factor and interleukin-6 are correlated with macular edema in branch retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 2006;244(3):309-315.
- Noma H, Funatsu H, Mimura T, Eguchi S, Shimada K. Inflammatory factors in major and macular branch retinal vein occlusion. Ophthalmologica. 2012;227(3):146-152.
- Noma H, Funatsu H, Mimura T, Harino S, Hori S. Vitreous levels of interleukin-6 and vascular endothelial growth factor in macular edema with central retinal vein occlusion. Ophthalmology. 2009;116(1):87-93.
- Park SP, Ahn JK, Mun GH. Aqueous vascular endothelial growth factor levels are associated with serous macular detachment secondary to branch retinal vein occlusion. Retina. 2010;30(2):281-286.
- Shimura M, Nakazawa T, Yasuda K, Kunikata H, Shiono T, Nishida K. Visual prognosis and vitreous cytokine levels after arteriovenous sheathotomy in branch retinal vein occlusion associated with macular oedema. Acta Ophthalmol. 2008;86(4):377-384.
- Takahashi E, Hirata A, Inomata Y, Kawaji T, Fukushima M, Tanihara H. Erythropoietin and vascular endothelial growth factor in the vitreous fluid of patients with various vitreoretinal diseases. Invest Ophthalmol Vis Sci. 2003;44: ARVO E-Abstract 4870.
- Yasuda S, Kachi S, Ueno S, et al. Electroretinograms and level of aqueous vascular endothelial growth factor in eyes with hemicentral retinal vein occlusion or branch retinal vein occlusion. Jpn J Ophthalmol. 2014;58(3):232-236.
- Lu Q, Zou W, Chen B, Zou C, Zhoa M, Zheng Z. ANGPTL-4 correlates with vascular endothelial growth factor in patients with proliferative diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2016;254(7):1281-1288.
- Watanabe D, Suzuma K, Suzuma I, et al. Vitreous levels of angiopoietin 2 and vascular endothelial growth factor in patients with proliferative diabetic retinopathy. Am J Ophthalmol. 2005;139(3):476-481.
- Ran R. Du L, Zhang X, et al. Elevated hydrogen sulfide levels in vitreous body and plasma in patients with proliferative diabetic retinopathy. Retina. 2014;34(10):2003-2009.
- Baharivand N, Zarghami N, Panahi F, et al. Relationship between vitreous and serum vascular endothelial growth factor levels, control of diabetes and microalbuminuria in proliferative diabetic retinopathy. Clin Ophthalmol. 2012;6:185-191.
- Endo M, Yanagisawa K, Tsuchida K, et al. Increased levels of vascular endothelial growth factor and advanced glycation end products in aqueous humor of patients with diabetic retinopathy. Horm Metab Res. 2001;33(5):317-322.
- Mohan N, Monickaraj F, Balasubramanyam M, Rema M, Mohan V. Imbalanced levels of angiogenic and angiostatic factors in vitreous, plasma and postmortem retinal tissue of patients with proliferative diabetic retinopathy. J Diabetes Complications. 2012;26(5):435-441.
- Noma H, Funatsu H, Yamasaki M, et al. Aqueous humour levels of cytokines are correlated to vitreous levels and severity of macular oedema in branch retinal vein occlusion. Eye (Lond). 2008;22(1):42-48.
- Noma H, Yasuda K, Shimura M. Cytokines and the pathogenesis of macular edema in branch retinal vein occlusion. J Ophthalmol. 2019;2019:5185128.
- Regula JT, Lundh von Leithner P, Foxton R, et al. Targeting key angiogenic pathways with a bispecific CrossMAb optimized for neovascular eye diseases. EMBO Mol Med. 2016 Nov 2;8(11):1265-1288. Erratum in: EMBO Mol Med. 2019;11(5):e10666.
- Noma H, Yasuda K, Mimura T, Ofusa A, Shimura M. Relationship between retinal blood flow and cytokines in central retinal vein occlusion. BMC Ophthalmol. 2020;20(1):215. Published 2020 Jun 5.
- Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15(2):171-185.
- Noma H, Mimura T, Yasuda K, Shimura M. Role of soluble vascular endothelial growth factor receptors-1 and -2, their ligands, and other factors in branch retinal vein occlusion with macular edema. Invest Ophthalmol Vis Sci. 2014;55(6):3878-3885.
- Vabysmo (faricimab-svoa) full U.S. Prescribing Information. Genentech, Inc. October 2023.
- Campochiaro PA, Hafiz G, Mir TA, et al. Pro-permeability factors after dexamethasone implant in retinal vein occlusion; the Ozurdex for Retinal Vein Occlusion (ORVO) study. Am J Ophthalmol. 2015 Aug;160(2):313-321.e19.
- Ip M, Hendrick A. Retinal Vein Occlusion Review. Asia Pac J Ophthalmol (Phila). 2018 Jan-Feb;7(1):40-45. doi: 10.22608/APO.2017442. Epub 2017 Dec 27.
- LUCENTIS® (ranibizumab) Injection full U.S. Prescribing Information. Genentech, Inc. February 2024.
- Data on file. Regeneron Pharmaceuticals, Inc.
- EYLEA® (aflibercept) Injection full U.S. Prescribing Information. Regeneron Pharmaceuticals, Inc. December 2023.
© 2024, Regeneron Pharmaceuticals, Inc. All rights reserved.
US.EYL.24.07.0004 08/2024

