Announcer:
You’re listening to Project Oncology on ReachMD, and this episode is sponsored by Exact Sciences. This is a non-certified educational series produced and controlled by ReachMD. This series is intended for healthcare professionals only. This program discusses a technology under development. Any features discussed describe current development goals. It has not been cleared or approved by the U.S. FDA or any other national regulatory authority. Here’s your host, Dr. Charles Turck.
Dr. Turck:
This is Project Oncology on ReachMD. I’m Dr. Charles Turck, and joining me to discuss the poster he co-authored that was presented at the 2022 American Association for Cancer Research Special Conference on Precision Prevention, Early Detection, and Interception of Cancer is Dr. Frank Diehl. Dr. Diehl is the Senior Vice President of Multi-Cancer Early Detection at Exact Sciences Corporation, and his poster presented findings on the performance of a multi-analyte early cancer detection test. Dr. Diehl, thanks for being here today.
Dr. Diehl:
Thank you.
Dr. Turck:
Now if we start with some background, Dr. Diehl, would you tell us about the unmet need in cancer screening and about multi-cancer early detection, or MCED, tests?
Dr. Diehl:
Yeah, sure. So most importantly, cancer screening is an approach to find the cancer early before it is symptomatic and when the clinical intervention is most likely to be effective. So this means cancer screening can save lives. So currently, there are screening recommendations by the United States Preventative Services Taskforce for four different cancer types: lung, breast, colorectal, and cervical cancer. And there are multiple approaches available to screen for these cancer types. The unmet need in cancer screening is that there are no recommended screening options available for the other cancer types that account for roughly two-thirdsof the cancer death. And also, even for the screening options for the four major cancer types that I mentioned, there’s still room to increase the adherence to screening.
Multi-cancer early detection tests may help with this unmet need by offering a unique approach to cancer screening because the tests are designed to utilize a single blood draw and to detect cancer signals across multiple cancer types. What it means is that the MCED tests might address several of these unmet needs. So first, there’s the need to screen for multiple cancers without a recommended screening option. Second, this test can complement current recommended single-organ screening methods. And lastly, because this is a blood test, it may help to access the screening of a broader population, for example, underserved populations.
Dr. Turck:
And as a follow-up to that, I thought I’d see if you had any other thoughts on the role or potential of a multi-biomarker MCED test.
Dr. Diehl:
Yeah. We believe that the ability to detect multiple cancer types at an early stage with a single blood test is mainly driven by the utilization of a broad range of organelle tumor-specific biomarkers. And why do we think that way? So first, now we understand that multiple molecular parts RAS are altered during cancer development, and it affects different genes. Second, the type of alterations can be very heterogenous within or between tumor types. And lastly, the mechanism by which the tumor-specific biomarkers are released into the blood stream can also vary; for example, a tumor DNA molecule might be released differently into the blood stream than a protein biomarker. Because of all of these different factors, we believe that a multi-biomarker MCED test has the highest chance of detecting a broad range of tumors at various stages.
Dr. Turck:
Now if we zero in on your poster, what was the main objective of your research and how did you go about achieving that objective?
Dr. Diehl:
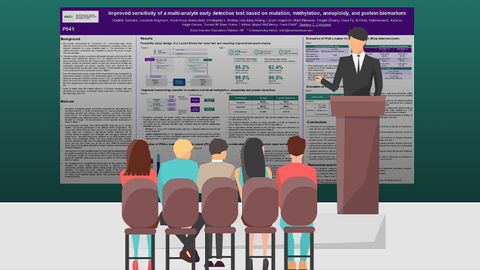
Yeah. Our overarching research objective is to design a multi-cancer early detection test that has a high but clinical meaning for sensitivity while maintaining a high clinical specificity to limit the number of false positives. In particular, the research that we are presenting here was built on an earlier clinical feasibility study that was presented at the 2022 Annual Conference of the European Society for Molecular Oncology. And the main objective of this research was to improve the sensitivity of our multi-biomarker class test by making changes and improvements to the biomarker-calling algorithms and to apply machine learning to the calling itself. Additionally, we tested the impact of PSA with a newly developed cutoff to evaluate the potential to increase the detection of clinically actionable prostate cancer. We have approached this objective by designing a retrospectively assembled case-controlled study to train, validate, and test our cancer-calling algorithms for two different test configurations. One of the test configurations included three biomarker classes comprised of methylation, aneuploidy, and protein biomarkers, and the second was a four-biomarker class test design that is comprised of the same markers as the three-biomarker class test plus somatic mutations. We tested a cancer cohort that included cancer types across all stages and 15 different organ types that are frequently found in the public, and we also looked at a control cohort that included non-cancer subjects and some enrichment of individuals with non-cancerous and benign tumors.
Dr. Turck:
For those just tuning in, you’re listening to Project Oncology on ReachMD. I’m Dr. Charles Turck, and I’m speaking with Dr. Frank Diehl about the poster he co-authored at the 2022 AACR Special Conference on Precision Prevention, Early Detection, and Interception of Cancer.
With that background in mind, Dr. Diehl, let’s turn our attention to results. What were the main findings regarding the performance of the three versus four-biomarker class MCED tests?
Dr. Diehl:
We found that both the three- and four-biomarker class test configuration was able to detect the cancers in all of the organ sites we analyzed across all stages tested. So more specifically, when we compared the three with the four-biomarker configuration, we found that adding the somatic mutations in the four-biomarker class test design helped to increase the overall sensitivity to 62.4 percent at 98 percent specificity in comparison to a 55.2 percent sensitivity. So overall, the increase of sensitivity of 7 percent was observed with a minimal loss of specificity. So most importantly, the increase observed with the four-biomarker class test design was strongest in early-stage cancers. So with that, the combination of these biomarkers we found for stage 1 and 2 cancers was 40.5 percent sensitivity, which was a 9 percent increase over the three-biomarker configuration.
Dr. Turck:
And what impact might a future MCED test have on cancer screening if it were able to deliver performance characteristics like those demonstrated in your study?
Dr. Diehl:
Yeah. The result of the study demonstrates the potential of a multi-cancer early detection test, and it could create a paradigm shift in cancer screening such that a test could detect cancers where no recommended screening options exist today, and it would complement, not replace, existing single-organ screening options. With the added sensitivity of the four-biomarker class test design, there is also potential to detect more early-stage cancers when there is a higher chance of a cure to intervention. So over time, MCED tests, in general, might have the potential then to make an impact on the overall cancer burden.
Dr. Turck:
And if we bring this all together before we close, Dr. Diehl, what are the main conclusions you’d like our audience to take away from your research?
Dr. Diehl:
So first, we show that a multi-biomarker class test that tests different analytes and tests different cancer-specific alterations has a high chance to detect a broad range of cancers at all stages. And we also believe that this is particularly important for early cancers as they are usually smaller and tend to release less of the tumor-specific content in the circulation. Our four-biomarker test configuration using aneuploidy, methylation mutations, and proteins provides a complimentary system for a multi-cancer detection test. When we compared this result to the three-biomarker test design, we demonstrated a notable improvement in stage 1 and 2 cancer detection. We tested 15 different organ sites, which represent about 76 percent of all cancer deaths, and so our multi-biomarker test design detected these cancers at all stages. So specifically, the four-biomarker test was performing very well at greater than 62 percent at 98 percent specificity.
Ultimately, the takeaway is that MCED tests have the potential to expand the screening options to a broad range of cancers where currently no screening options exist and has the potential to enable curative interventions that may help to reduce the overall tumor burden.
Dr. Turck:
Well as that brings us to the end of today’s program, I want to thank my guest, Dr. Frank Diehl, for joining me to discuss the findings from his research on a multi-analyte early cancer detection test. Dr. Diehl, it was great having you on the program today.
Dr. Diehl:
Thank you.
Announcer:
This episode of Project Oncology was sponsored by Exact Sciences. To access this and other episodes in this series, visit ReachMD.com/Project Oncology, where you can Be Part of the Knowledge. Thanks for listening!






Facebook Comments